
If you’ve been told you have osteoarthritis of the spine – or you suspect you might – you’re not alone. This condition ranks among the most common causes of chronic neck and low back pain in adults, particularly those over 40. My guide covers everything you need to know, from understanding what’s happening in your spine to practical treatment options that can help you get back to daily life.
What Is Osteoarthritis of the Spine?
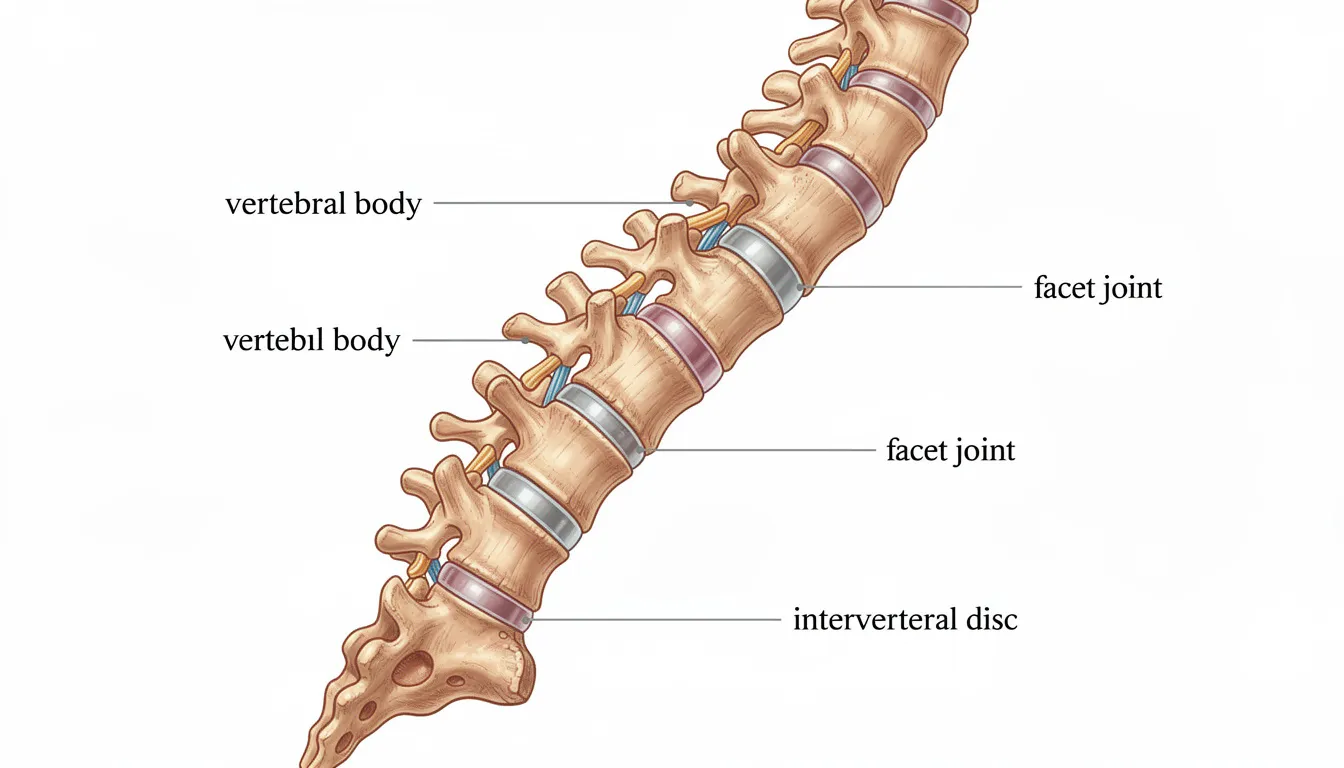
Osteoarthritis of the spine is a degenerative joint disease that primarily affects the facet joints: small joints located between and behind your vertebrae that allow your spine to bend and twist. In some cases, the intervertebral discs (the cushioning pads between vertebrae) are also affected. Osteoarthritis can occur in different regions of the spine, including the cervical, thoracic, and lumbar areas, affecting movement and nerve function.
Here’s what’s happening inside your spine:
- Vertebrae are the individual bones stacked to form your spinal column
- Facet joints connect these vertebrae and guide spinal movement
- Intervertebral discs act as shock absorbers between vertebrae
- The spinal cord runs through a canal formed by the vertebrae, with nerve roots branching out at each level
As discs degenerate and narrow, the space between the spinal joints also narrows. The narrowing of the disc results in narrowing of the space between the spinal joints, which can increase weight-bearing forces on the joints and lead to osteoarthritis. Over time, the cartilage covering the facet joints becomes thinner and rougher. When this protective layer wears away, bones can rub together, creating friction and inflammation. Your body responds by forming bone spurs (osteophytes) along the edges of vertebrae—a repair attempt that can sometimes cause additional problems. These degenerative changes can lead to nerve compression and pain, which often lead to radiating symptoms and impairment.
In a healthy spine, facet joints carry about 33% of the body’s weight load. The lumbar spine, which bears most of the body’s weight, is particularly susceptible to degeneration. As osteoarthritis develops, this responsibility can increase dramatically to 70%, accelerating the degenerative process.
Quick Terminology Guide:
- Spinal osteoarthritis: Specifically refers to wear-and-tear arthritis affecting spinal joints
- Spondylosis: A broader term for age-related degenerative changes throughout the spine
- Degenerative disc disease: Focuses on disc breakdown rather than joint changes
Osteoarthritis vs. Spondylosis and Other Spinal Conditions
“Spondylosis” is an umbrella term describing degenerative changes of the spine, including facet joint osteoarthritis, disc degeneration, and bony growths in the cervical, thoracic, or lumbar spine. While osteoarthritis of the spine is a key component of spondylosis, not all spinal degeneration causes symptoms. Degenerative spondylolisthesis, caused by osteoarthritis of the facet joints, most frequently affects people age 50 and older.
Understanding the differences between spinal arthritis types helps clarify your diagnosis:
Condition | Key Characteristics |
|---|---|
Osteoarthritis | Wear-and-tear degeneration; affects facet joints; develops gradually with age; commonly affects weight-bearing joints such as the hips, knees, and hands |
Rheumatoid arthritis | Autoimmune; inflammatory; typically affects multiple joints symmetrically |
Ankylosing spondylitis | Inflammatory spinal arthritis; can fuse vertebrae together over time |
Herniated disc | Focal disc issue; not necessarily related to overall joint wear |
Location matters for symptoms:
- Cervical spine (neck): Pain, stiffness, headaches, and symptoms radiating to the shoulder and arms
- Thoracic spine (mid-back): Less common; sometimes related to posture or prior injury
- Lumbar spine (low back): Very common; lumbar spine osteoarthritis can cause leg pain from nerve root compression. Bone spurs and narrowing of the spinal canal can increase pressure on nerves and surrounding tissues, leading to pain, numbness, or weakness.
Causes and Risk Factors
Spinal osteoarthritis develops gradually over years due to mechanical “wear and tear” combined with age-related disc dehydration and cartilage breakdown. Think of it like the gradual wearing of brake pads in a car—use over time takes a toll.
Non-Modifiable Risk Factors:
- Age over 40–50 years (prevalence rises significantly after 60)
- Female sex (slightly higher risk after menopause)
- Family history of osteoarthritis or spinal degenerative disease
Modifiable Risk Factors:
- Obesity or excess weight, which increases load on the lumbar spine
- Repetitive spinal loading from occupations (construction, nursing, warehouse work) or high-impact sports
- Prior spinal injuries, fractures, or surgery that alter normal biomechanics
- Poor posture and sedentary lifestyle
- Smoking (reduces blood flow and disc nutrition)
Other conditions like scoliosis can also contribute to uneven joint space distribution and accelerated wear on specific spinal joints.
Symptoms: How Osteoarthritis of the Spine Feels
The main symptoms of spinal osteoarthritis typically begin slowly and worsen over time. Here’s what most people experience:
Typical Pain Patterns:
- Deep, aching pain in the neck or lower back, often worse after activity or prolonged standing
- Morning stiffness that improves after 20–30 minutes of gentle movement
- Pain that may flare with weather changes or heavy lifting
Mechanical Nature of Symptoms: Pain caused by spinal osteoarthritis often worsens with extension movements—bending backward or standing upright for long periods. Many people find relief when sitting, bending slightly forward, or leaning on a shopping cart. This pattern often suggests that bone spurs are narrowing the spinal canal.
Nerve-Related Symptoms: When bony growths or thickened ligaments compress nerves, you may experience:
- Radiating pain, burning, or “electric” sensations into arms (cervical involvement) or legs (lumbar involvement)
- Numbness, tingling, or weakness following specific nerve root distributions
- Pain extending below the knee in lumbar cases often indicates nerve root compression
Red-Flag Symptoms Requiring Urgent Care:
- Sudden, severe weakness in arms or legs
- Loss of bowel or bladder control, or numbness in the saddle area (possible cauda equina syndrome)
- Fever, unexplained weight loss, or new back pain with a history of cancer
These emergency symptoms require immediate medical evaluation.
When and How to Seek Medical Care
See a doctor if:
- Back or neck pain lasts more than 4–6 weeks
- Pain interferes with sleep, work, or daily activities
- Over-the-counter medications and rest are no longer effective
- You experience numbness, weakness, or other neurologic symptoms
Specialists You May Encounter:
- Primary care doctors for initial evaluation
- Rheumatologists for inflammatory arthritis concerns
- Orthopedic spine surgeons or neurosurgeons for surgical consultations
- Physical therapists for rehabilitation and exercise programs
Before Your Visit, Prepare:
- A symptom diary noting onset, triggers, and what helps
- List of current medications and prior imaging or surgeries
- Key questions about diagnosis and treatment options
Most cases can be managed without surgery in outpatient settings. Hospital admission is rarely needed unless severe neurologic deficits are present.
Testing and Diagnosis
Diagnosis of facet joint osteoarthritis combines clinical assessment with imaging. Your doctor may use:
- Detailed medical history
- Physical examination
- Imaging tests (X rays, MRI)
- Occasionally, nerve studies
Importantly, mild radiographic changes are common with age and don’t always correlate with pain. Imaging findings must be interpreted alongside your symptoms to determine what’s actually causing problems.
Medical History
Your doctor may ask about:
- Location, intensity, and character of pain (dull, sharp, burning)
- Duration and daily pattern of symptoms
- Activities that make pain worse or provide relief
- Presence of numbness, tingling, or weakness in arms or legs
Expect questions about prior injuries, spinal surgeries, occupational strain, and sports participation. Your doctor should also review other health conditions (diabetes, osteoporosis, inflammatory arthritis) and medications you take.
This conversation typically takes 5–15 minutes and guides which tests are needed.
Physical Examination
During the physical examination, your doctor may:
- Inspect posture, spine alignment, and gait
- Test range of motion in your neck and low back (bending forward, backward, and side-to-side)
- Assess which movements reproduce your pain
Neurologic Exam Components:
- Strength testing in muscles of the arms and legs
- Reflex checks at the knees, ankles, and biceps
- Sensation testing with light touch or pinprick along dermatomes
Specific maneuvers like Spurling’s test (for cervical radiculopathy) or straight-leg raise (for lumbar involvement) help identify nerve compression.
X-rays
Plain X rays are often the first imaging test ordered for chronic neck or low back pain lasting more than several weeks.
What X-rays Show:
- Narrowing of joint space and disc height loss
- Bone spurs along vertebral edges and affected joints
- Misalignment or abnormal curvature (such as scoliosis)
Limitations: X-rays don’t visualize nerves or soft tissues well but are useful for assessing overall structure and degree of degeneration. They’re quick, inexpensive, involve low radiation exposure, and are usually taken in standing positions to evaluate load-bearing alignment.
MRI Scans
MRI provides detailed images of soft tissues, including intervertebral discs, the spinal cord, nerve roots, and ligaments.
When MRI Is Ordered:
- Persistent pain despite conservative care
- Neurologic symptoms such as numbness, weakness, or significant radiating pain
- Suspicion of spinal stenosis, disc herniation, infection, or tumor
What MRI Reveals:
- Disc degeneration, bulging, or herniation
- Nerve root compression from bone spurs or thickened ligaments
- Severity of spinal canal narrowing
MRI typically takes 20–45 minutes, is painless, and doesn’t use radiation. Alternative imaging options exist for patients with certain implants or severe claustrophobia.
Electromyogram (EMG) and Nerve Conduction Studies
EMG and nerve conduction studies measure nerve and muscle function to identify pinched or damaged nerves.
When These Tests Are Ordered:
- Unexplained weakness, numbness, or tingling in arms or legs
- Imaging results don’t fully explain neurologic symptoms
The Procedure:
- Small electrodes on the skin measure nerve conduction
- Thin needle electrodes are inserted into selected muscles to record electrical activity at rest and during gentle contraction
Testing typically takes 15–45 minutes and may cause temporary discomfort. Results help evaluate whether nerve root involvement matches the suspected spinal level.
Non-Surgical Treatment Options
Most people with osteoarthritis of the spine can be managed without surgery. Treatment combines lifestyle changes, physical therapy, and medications tailored to your age, overall health, severity of degeneration, and personal goals.
The main conservative treatment pillars include:
- Physical therapy and exercise
- Medications for pain and inflammation
- Targeted injections
- Self-care and lifestyle modifications
Physical Therapy and Exercise
Physical therapy is central to managing spinal arthritis. A physical therapist will evaluate your posture, movement patterns, flexibility, and muscle strength to design a personalized program.
Key Components:
- Core and hip strengthening exercises for lumbar spine osteoarthritis
- Neck and upper back strengthening for cervical involvement
- Flexibility work for hamstrings, hip flexors, and thoracic spine
- Manual therapy techniques (joint mobilization, soft tissue work) to reduce stiffness

Home Exercise Programs:
- Gentle daily stretching
- Low-impact aerobic activities like walking, cycling, or swimming
- Balance and stability exercises to reduce fall risk
Research shows weight-bearing exercises significantly increase lumbar spine bone mineral density. Strengthening exercises help muscles support spinal joints rather than allowing tight muscles to overload them.
Medications
Over-the-Counter Options:
- NSAIDs such as ibuprofen and naproxen for pain and inflammation (use cautiously with stomach, kidney, or heart concerns)
Prescription Options When Needed:
- Stronger NSAIDs or topical NSAIDs (gels, creams) for localized pain
- Short courses of muscle relaxants for acute muscle spasm
Long-term opioid use is generally discouraged for chronic spinal osteoarthritis due to dependence and side effect risks. These medications should be reserved for select cases under close medical supervision.
Always discuss all medications and supplements with your doctor, especially if you have other conditions or take blood thinners.
Injections and Other Interventions
Common Injection Options:
- Facet joint injections: Local anesthetic and corticosteroid to reduce inflammation and confirm the pain source
- Medial branch nerve blocks: Can be followed by radiofrequency ablation for longer-term relief
- Epidural steroid injections: Used when nerve root inflammation from bone spurs or disc degeneration causes radiating limb pain
Studies suggest epidural injections may provide short-term improvements in pain and quality of life for up to two weeks. Injections are typically performed under fluoroscopic or ultrasound guidance in outpatient settings.
Relief may be temporary (weeks to months), so injections are often combined with physical therapy to maximize long-term benefit.
Self-Care, Lifestyle, and Home Management
Weight Management: Reducing excess weight decreases stress on the lumbar spine and can significantly improve pain over time.
Activity Modification:
- Avoid prolonged sitting or standing; change positions regularly
- Use proper body mechanics when lifting, pushing, or pulling
Practical Tools and Strategies:
- Heat (showers, heating pads) for morning stiffness
- Ice packs for flares of sharp pain after activity
- Supportive chairs and proper screen height at work
- Sleep positioning strategies (pillow between knees for side sleepers)

Smoking cessation and alcohol moderation support bone and disc health. Small daily adjustments in activity levels can prevent flares and maintain mobility.
Surgical Treatment: When Is Surgery Considered?
Surgery for osteoarthritis of the spine is relatively uncommon and reserved for specific situations where conservative treatment hasn’t worked.
Main Indications for Surgery:
- Progressive neurologic deficits (worsening weakness, loss of coordination)
- Severe spinal stenosis causing disabling leg or arm symptoms
- Intractable pain significantly limiting daily activities despite months of non-surgical care
- Cauda equina syndrome (a surgical emergency)
Common Procedures:
- Decompression surgery (laminectomy, foraminotomy): Removes bone or tissue pressing on nerves
- Spinal fusion: Stabilizes segments with severe degeneration or instability
Surgical decisions are influenced by age, overall health, bone quality, and patient preferences. Seeking a second opinion is often appropriate before major spinal surgery.
Living With Osteoarthritis of the Spine and Follow-Up Care
Spinal osteoarthritis is a chronic condition, but it can often be managed effectively with an ongoing plan that combines lifestyle changes, exercise, and periodic medical review.
Typical Follow-Up:
- Regular visits with your primary care doctor or specialist to adjust medications and monitor symptoms
- Check-ins with a physical therapist to update exercise routines and address new limitations
Practical Long-Term Strategies:
- Set realistic activity goals and pace tasks throughout the day
- Develop a flare-up plan (temporary rest, medication adjustment, heat/ice) agreed upon with your clinician
- Maintain a symptom diary to identify patterns and triggers
- Strengthen your core consistently to support spinal joints
Engaging with credible educational resources and support groups for people with arthritis and chronic back pain can provide valuable community based population insights and emotional support.
The key to living well with this condition is collaboration with your healthcare team, staying active within your limits, and focusing on what you can control. With the right approach, most people maintain meaningful mobility and quality of life for years to come.
