The Ageing Spine
What happens to the discs between the vertebrae as we get older?
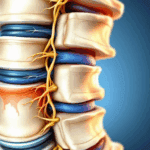
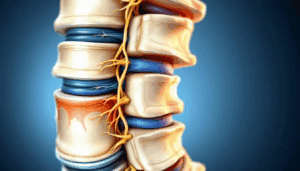
The intervertebral discs are the cushions or shock absorbers between the bones of the spine. As children and young adults our discs contain a lot of water. As we age disc nutrition becomes impaired, waste products build up within the disc, and less water is contained within the disc.
Consequently the disc loses thickness and is less able to withstand the mechanical loads going through the spine. This is a normal ageing process but can lead to common problems such as back pain and ‘slipped discs’ with sciatica.
Interesting fact: Water is also squeezed out of the discs over the course of a day when we are upright and goes back into the discs at night when lying down. This is why we are taller first thing in the morning when we get up than at the end of the day.
What conditions can arise as we age?
- Back pain – often first starts in young adults between 20-40 years old with episodes increasing in frequency to about age 65. About 85% of us will suffer with back pain at some stage in our lives. The spine has a tendency to stiffen after about 65 years with decreasing back pain.
- ‘Slipped disc’ – disc herniation, disc protrusion etc all means the same thing. Most common in young adults this involves the central part of the disc escaping through a weakness or tear in the wall of the disc. This can cause back pain and if a nerve is also pinched pain down the leg with pins and needles and numbness referred to as sciatica.
- Facet joint pain – the small joints behind the spine will inevitably develop ‘wear and tear’ changes (osteoarthritis) to some extent as we age. This is a common cause of back pain.
- Spinal stenosis – this is narrowing of the bony canal or holes through which the nerves run. Often caused in older age by a combination of factors such as narrowing of the disc, enlargement of arthritic facet joints, bony spurs, etc
What are the most common age-related back problems?
Back or neck pain arising from ‘wear and tear’ (osteoarthritis) in discs and facet joints.
Arm or leg pain caused by pinched nerves in the neck or lower back.
Spinal stenosis – older patients generally with leg symptoms brought on by standing and walking.
How can you keep your spine healthy as you age?
The rate at which our spines age is mostly predicted by our genetics ie. our parents. Lifestyle and other medical conditions such as diabetes contribute to a much lesser degree. Longterm smoking is detrimental to our discs and just about everything else!
We can’t change our genetics but there are things which we can do to help our backs and reduce the impact of these degenerative changes. These include:
- Regular exercise particularly brisk walking.
- Avoid sitting for longer than 30 minutes. Get up and move frequently.
- Healthy diet and maintaining hydration (drink water) throughout the day.
- Exercises to strengthen the core muscles of the back and tummy which become increasingly important for our spine as we age.
- Avoid very heavy lifting or repetitive lifting jobs.
- Don’t smoke
What do you suggest for back pain and what do you advise against?
For an acute episode of back pain:
The Do’s
- simple analgesia such as paracetamol and an anti-inflammatory painkiller such as ibuprofen taken maximally and continuously if tolerated over 1-2 weeks. Codeine phosphate can be added if required and all these medications are available over the counter at a chemist without prescription. The pharmacist can advise further if necessary.
- A few days of rest may be necessary but the general advice is try and keep moving if possible.
- Gentle stretching exercises as pain allows. A physiotherapist may help with this if necessary.
- Gentle manual therapy may also be helpful for some during an episode of back pain but should not be continued as a ‘maintenance’ treatment when better.
- Do regular daily exercises to strengthen the core back and tummy muscles when better to reduce the frequency and severity of future back pain episodes. Consider joining a Pilates or Yoga group.
The Dont’s
- Avoid spending the day in bed without moving. This can slow recovery.
- Don’t panic and rush straight to the GP or worse A and E unless the pain is unmanageable or there are other causes for concern.
- Don’t stress out! Most episodes of back pain resolve within a few weeks so remain optimistic.
- Avoid having repeated sessions of manual therapy ad infinitum. If manual treatment is not helping within a few sessions, stop.
- Avoid online searches for ‘back pain cures’ and follow mainstream advice.
- Avoid lay theories of friends or family, however well intentioned, unless experienced in back pain care.
- Don’t self arrange MRI scans. Specialists should arrange specialist imaging as they know what to request and are trained to understand explain what the imaging shows and what is relevant or not. MRI scans show anatomy not pain so skilled interpretation is vital.
When is surgery an option?
Surgery is seldom required for back pain and should always be considered a last resort when nothing else has worked. Surgery generally works best when nerves are pinched (spinal stenosis) or if there is spinal instability (excess movement) or deformity.
A very simple earlier option for back pain (which is not improving with time, analgesia and exercise) are spine injections. The principal here is targeting the area of the back where the pain is thought to be arising with a strong anti-inflammatory (steroid) painkiller.
Injections can work very well in some individuals and speed a rapid recovery but may not work or last in others. Spine injections are carried out by spine specialists (often Consultant Spine Surgeons) with the best knowledge and understanding of spinal anatomy and diagnosis. Specialists will first arrange appropriate imaging of the spine to help make a diagnosis and then target injections if this seems a helpful option. Usually injections do not need to be repeated. Injections will often help facilitate better back rehabilitation and exercise.